 National Portal Of India
National Portal Of India 
Does India Need New Strategies for Improving Urban Health and Nutrition?
Urban situation: India faces a unique development paradox of being in the front ranks of fast growing global economies. Recent decades have seen unprecedented population growth in urban areas- every year about 7.5 million population is added to urban areas. According to UNs’ prognosis in 2011, India will nearly triple its population from 367 million in 2010 to 915 million in 2050. Urbanization is a complex and dynamic demographic phenomenon, which interacts with globalization, economic growth, income inequality, climate change, health and sustainability.
Urban populations have limited access to healthcare facilities especially when it comes to primary care in India. For example- NCT Delhi has merely eight Primary Health Centres (PHCs), no Community Health Centres (CHCs) and 134 tertiary care hospitals, which includes general as well as speciality, super and multi-speciality hospitals. Apart from these there are 33 dispensaries which do not have any inpatient facility but only observation beds. The layer of primary health care system in urban areas is not as impressive as in rural areas. There are considerable challenges in reaching the poor and marginalized communities in urban areas and ensuring equitable health outcomes.
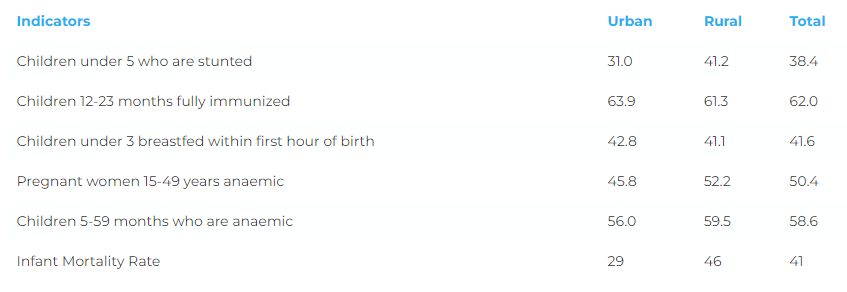
The policy focus so far has been mostly in rural and tribal areas on improving access to health services and strengthening the health systems. What’s been ignored are the poor and the marginalized in the urban areas facing the perils of ill-health whose numbers are multiplying by the day. The health and nutrition indicators in urban areas are as bad as of their rural counterparts. According to NFHS IV, 38% of urban poor children under five years are stunted. The Urban poor which is 26% of total urban population has even worse health and nutrition outcomes as a result of lack of adequate services. Almost 36% of urban children miss full immunization; which is as high as 58% amongst the urban poor.
Urban population contributes to 65% of India’s GDP which will jump to 70-75% in 2020 (Barclay’s report 2014). The GDP per capita income for urban (Rs 56,347 pa) is almost double as that of and rural (Rs 30,342). In spite of this stark difference in economies, the health and nutritional status of urban areas is as poor as that of rural; in fact status of urban poor is worse than rural poor!
Inadequacy in Public Health Delivery system: Poor health seeking behaviour leads to poor Health and Nutritional outcomes has been established by researchers and practitioners. Urban population, largely the poor and the marginalized, are “ghettoized” and “spaced out” because of the inadequacy in urban public health delivery system to reach them on account of location, their place of work such as constructions sites etc. In addition, ineffective outreach and weak referral system limits their access. Migrant population’s ability to navigate the complex landscape of deeply fragmented health system has made them much more vulnerable to the ill-effects of health. Lack of economic resources and health insurance inhibits their access to the available private facilities.
Empowering Urban Governance: Urban governance matters the most in effective delivery of health services. Multiple incarnations have taken place in name of urban health policy since 1990s; yet Urban Local Bodies (ULBs)-the third layer of democracy remain weak in focus as well as delivery of health and nutrition services. The 74th Amendment (also known as Nagarpalika Act) was framed for strengthening public health capacity of ULBs in 1992. This has not happened in its truest form. The Fifteenth Finance Commission must institutionalize the devolution process to ULBs so that, the funds flow from State Government is timely and effectively used. ULBs should be encouraged and empowered to enhance their revenue generating capacity in these functional areas and build their capacities to use these resources on providing more such services. Empowering ULBs with better financing options will overcome human resources challenges both for- implementation and monitoring.
Translating the rural health system approach into urban areas is not where a solution lies; but what we need is a new approach to tackle the complex and complicated urban health scenario. In 2013, Central Government realised this challenge and National Urban Health Mission (NUHM) was launched in the country. NUHM has systematically worked towards meeting the regulatory, reformatory, and developmental Public Health priorities. However, there is huge shortage of primary healthcare services in the urban areas and the scope of primary care should expand to preventive and promotive healthcare services along with curative. Linkages between ICDS and Health services need to be explored. There are NGOs which have successfully implemented these unified approaches in Urban areas- eg: SNEHA (Mumbai) runs Maternal and Child Nutrition model successfully by involving volunteers who dedicates two hours per week for community outreach. Moreover, the Mohalla clinics (Primary Health Centres) - an initiative of Delhi State Government is an aspirational model that provides a basic package of essential health services including medicines, diagnostics, and consultation free of cost. Several ULBs of Mumbai, Surat, Ahmedabad, etc have made concerted efforts to focus on both Health and Nutrition centres. Similar models/ ideas can be systemized with policy focus to encourage them and build on their efforts.
Need of the hour: What we need in complex urban settings is a multi-pronged approach- a new unified strategy for improving Health and Nutrition! The focus should be on- Extending and Strengthening the Primary care delivery mechanism which will be one point centre for preventive, promotive and curative services. Community awareness for the same in urban community can be generated through Jan Andolan, for improved service delivery and Outreach. The HWC platform can be leveraged to integrate Nutrition component through sensitization, counselling, rehabilitation, etc. Similar unified approaches need to be supported by and coordinated with other Non-Health sectors such as-Housing and Urban Development, Environment, Road transport, Education, Water and Sanitation, as well as CSRs, NGOs, Development partners and experts. It should cover all vulnerable population suffering from ‘urban penalties’ viz- pavement dwellers, rag-pickers, street children, rickshaw pullers, construction/ brick/ lime kiln workers, sex workers, and other temporary migrants, etc. Public health thrust should be on food & nutrition, NCDs, mental health, sanitation, clean drinking water, vector control, etc. Moreover, since one size doesn’t fit all- disruptive models (similar to few NGOs and ULBs described earlier) according to demographic and cultural variations of all States should be explored so that all citizens enjoy health, nutrition and wellbeing.
*Alok Kumar is Adviser and Khushboo Saiyed is a Young Professional, NITI Aayog. Views expressed are personal. With inputs from Nina Badgaiyan, Consultant, NITI Aayog.
*Data credits: WHO, World Bank, Census, NFHS, IIHS, NUHM Guidelines, Global Panel urbanization Policy Brief 9, Barclay’s report
*Image credits: UHRC and CINI